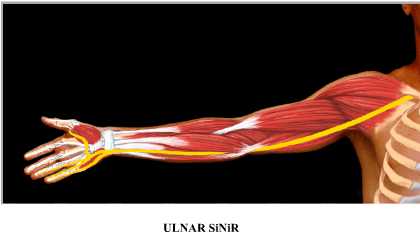
Ulnar Nerve Entrapment
When you hit your elbow somewhere and feel an electrical current or pain spreading to your entire arm, you feel your ulnar nerve. However, sometimes this picture created by the ulnar nerve can be permanent and can create a picture that disturbs the fingers and wrist. The ulnar nerve extends along the entire arm and ends by passing the elbow and wrist. It is responsible for the sensation of the little finger and ring finger of the hand and part of the movement of the fingers of the hand. It passes through a tunnel that you can feel with your hand on the inner side of the elbow. If the ulnar nerve is affected by a trauma to the elbow (such as after elbow fractures), the nerve is compressed in this tunnel due to the edema that develops in the nerve. This picture is called cubital tunnel syndrome or ulnar nerve compression syndrome.
- Feeling of tension on the inside of the elbow
- A feeling of numbness in the little finger and ring finger of the hand, especially at night
- Numbness occurs after the elbow remains in a folded position for a long time, such as while driving or talking on the phone.
- Difficulty using a musical instrument or doing a task involving the fingers of the hand
- Feeling of weakness in grasping or sorting
- Complaints such as pain on the inner side of the entire arm may occur.
- Those who fall on their elbows
- People who work in jobs that require elbow movement (such as secretaries, drivers)
- Diabetics
- Those with arthritis problems or thyroid problems
- Alcoholics are at risk.
- Keeping the elbow as straight as possible to prevent nerve compression,
- Preventing arms from crossing over the chest,
- If you make frequent phone calls, create a system where you don't use your elbow (like talking into a megaphone)
- Adjust your desk to prevent your elbow from remaining in a bent position,
- Splints that adjust the position of the arm that you will use at night,
- Use of elbow pads to protect the elbow during sports
- Corticosteroid injection (to reduce edema)








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment